A practical guide for CTOs, IT heads, and compliance officers at hospitals, healthtech startups, diagnostic labs, and healthcare SaaS companies in India.
The Healthcare Cloud Problem Nobody Talks About in the Sales Deck
Suppose a radiologist in Pune opens a DICOM imaging file at 11:47 PM just before an emergency surgery. The file takes 40 seconds to load. The surgeon is waiting, and so is the patient.
This delay is not because something is broken. It comes from an architectural choice made much earlier, storing medical imaging data on a hyperscaler’s “India region” that, under real load at night, ends up routing traffic through infrastructure not optimised for this location, this workload, or this level of urgency.
Healthcare IT in India is in a tough spot. The data is extremely sensitive, regulations are getting stricter, workloads are heavy and unpredictable, and the impact of failure is serious, not just technical but real-world.
Still, many hospitals, diagnostic chains, and healthtech platforms rely on the same standard cloud setups used by e-commerce companies, mostly because they are not aware of better options designed for their needs.
A Real Scenario: The Diagnostic Chain That Discovered Its Cloud Wasn't DPDP-Ready
Picture a diagnostic chain with around 80 collection centres across Maharashtra and Karnataka. They have digitised everything, lab reports, ECGs, ultrasound images, and patient history. Their platform is solid, the engineering team knows what they are doing, and they are using a major hyperscaler’s Mumbai region, assuming that keeps their data within Indian jurisdiction.
Then their legal team reviews compliance under the DPDP Act 2023, and a few issues show up at once.
First, their cloud provider is based in the US. So even if the data is physically stored in Mumbai, it still falls under US CLOUD Act jurisdiction. This means a foreign request could potentially access Indian patient data without going through Indian courts.
Second, their storage costs have quietly grown to around ₹4.2 lakh per month, and a big chunk of that, nearly 60 percent, is due to egress. Radiologists across centres keep downloading DICOM files for reporting and second opinions, which adds up fast.
Third, a hospital partner asks for a written confirmation that patient data will never leave Indian legal jurisdiction. They are not able to give a clear answer.
This is not a poorly run startup. It is a well-managed healthcare business hitting the limits of infrastructure that was never really designed for healthcare compliance needs of India.
And this is not an isolated case. Similar situations are happening across many healthcare organisations in India, from diagnostic chains to telemedicine platforms and hospital systems. The compliance risks are real, the costs are rising, and the need for a better setup is becoming hard to ignore.
Why Generic Cloud Infrastructure Fails Healthcare Specifically
Healthcare has requirements that expose the gaps in generic hyperscaler infrastructure more sharply than almost any other sector.
The Data Sovereignty Gap
Patient data is one of the most sensitive categories under India’s DPDP Act. Frameworks like ABDM, the National Digital Health Blueprint, and other emerging regulations all send a clear signal, health data should be stored and processed within Indian legal jurisdiction, with accountability defined by Indian law.
When this data is stored on a US-headquartered cloud platform, the situation becomes less clear. Even if the data is physically located in India, it still falls under the legal reach of that company’s home country. This creates a grey area that compliance teams struggle to explain or justify.
The US CLOUD Act adds to this concern by allowing American authorities to request data from US cloud providers globally. That means Indian patient records are not automatically protected from such access, which raises serious questions for healthcare organisations handling sensitive data.
The Latency Cost in Clinical Contexts
In most industries, an extra 30ms of latency is just a small inconvenience for users. But in healthcare, even that delay can have real clinical impact. Workflows like radiology, real-time diagnostics, teleconsultations, and ICU monitoring depend on fast and reliable response times.
The problem is that standard cloud setups in India often struggle to meet these needs, especially in Tier 2 and Tier 3 cities where network conditions are already limited.
The Compliance Complexity
CERT-In's April 2022 directions require maintaining logs for 180 days within Indian jurisdiction. The DPDP Act establishes accountability for data fiduciaries. ABDM sets integration and data handling standards. NMC and state medical council guidelines are evolving. Running this on infrastructure governed by foreign law and without native India compliance documentation creates audit exposure at every level.
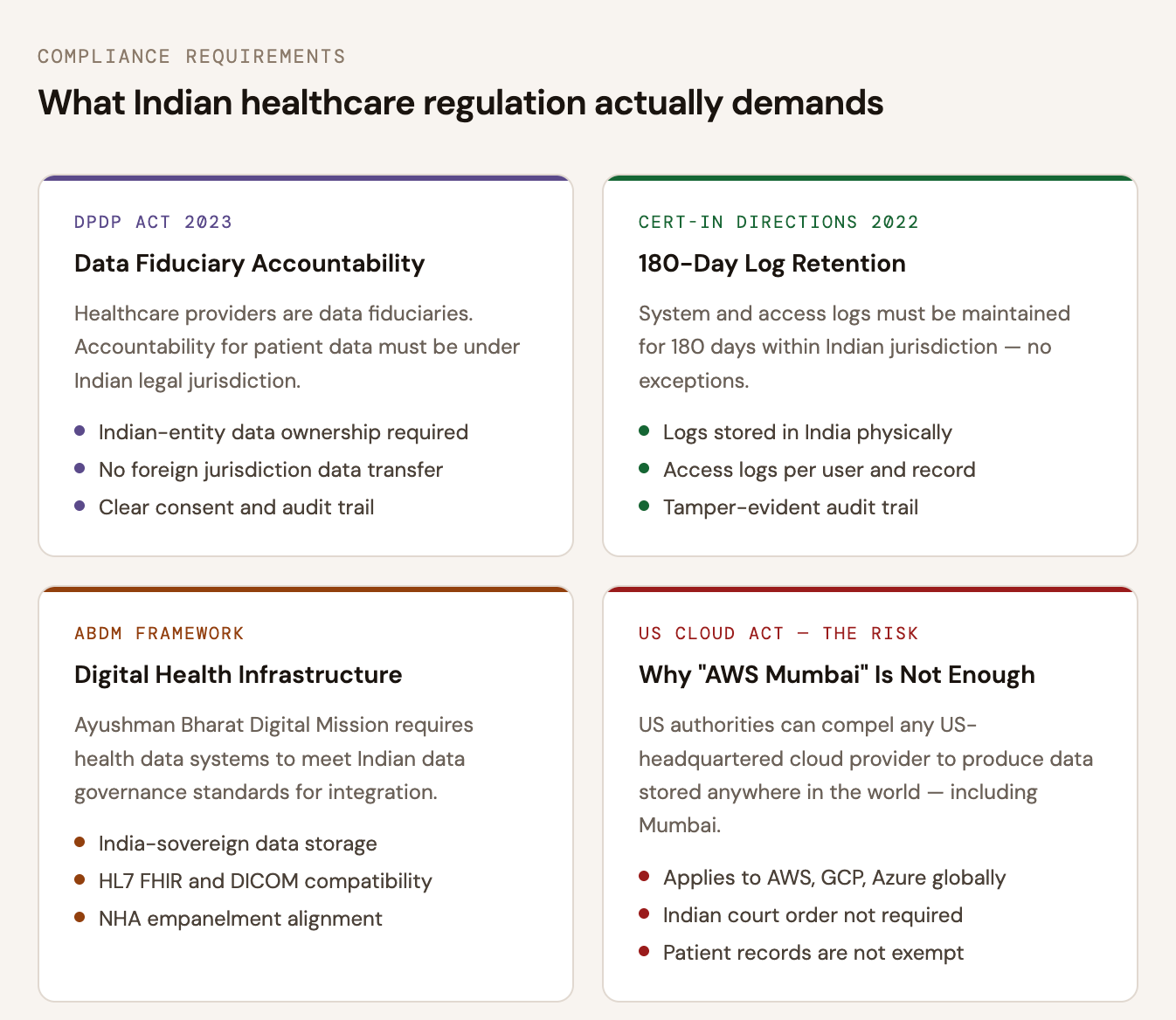
Four regulatory frameworks every Indian healthcare organisation must navigate.
The Cost Structure Doesn't Fit Healthcare Data Profiles
Healthcare data has a specific profile: large individual objects (DICOM files can be 50–500 MB each), high read frequency (reports accessed repeatedly across care teams), and long retention requirements (patient records must often be retained for 7+ years). On hyperscaler pricing, the combination of storage at scale plus egress on every access creates bills that grow non-linearly and unpredictably.
How IBEE’s Infrastructure Is Built for Healthcare Workloads
IBEE Hosting runs on Tier 4 certified data centres in India, which is the highest global standard for reliability. This is not just a configuration choice, it is a physical infrastructure difference that really matters in healthcare, where uptime directly affects patient care.
1. Tier 4 Reliability — 99.995% Uptime
Tier 4 means fully fault-tolerant systems with no single point of failure. Power, cooling, and networking all have redundancy, and even maintenance does not cause downtime.
For healthcare systems like EMR platforms or imaging archives, downtime is not just a technical issue, it impacts patient care. The difference between 99.995% and the typical 99.99% SLA may sound small, but it translates to about 26 fewer minutes of downtime per year, which can matter in critical situations.
2. 100% India-Sovereign Data
With IBEE, all data is stored on infrastructure owned and operated in India under Indian law. There is no exposure to foreign jurisdiction like the US CLOUD Act, and no ambiguity about where patient data legally resides.
This gives healthcare organisations something very important: a clean and clear data ownership story that aligns with DPDP Act, ABDM, and audit requirements.
3. Low Latency for Real Clinical Workflows
IBEE’s infrastructure is designed specifically for Indian network conditions. It is not just a global system with a local region added on.
For use cases like radiology reporting, teleconsultation, or multi-city diagnostic chains, this leads to noticeably better performance. When a radiologist opens multiple DICOM files in a shift, faster load times directly improve throughput and reduce delays in reporting.
4. Built-in Security for Healthcare
IBEE includes security features like AES-256 encryption at rest, TLS 1.3 in transit, IAM-based access control, versioning, and audit logs by default.
For healthcare teams, this means:
- Clear encryption standards for compliance
- Full access logs for audits
- Protection against accidental data loss
- Fine-grained access control across teams
All of this is available without needing separate add-ons.
5. Predictable Pricing for Long-Term Data
Healthcare data grows continuously and often needs to be stored for years. With many cloud providers, costs increase unpredictably due to egress charges, retrieval fees, and tier transitions.
IBEE keeps it simple:
- ₹1.5 per GB per month for storage
- ₹2 per GB for egress
- Uploads are free
- Internal traffic is free
There are no hidden retrieval charges or complex pricing tiers. What you store is what you pay for, consistently over time.
6. S3-Compatible, No Rebuild Needed
IBEE is fully S3-compatible, which means existing systems like HMIS, EMR, and PACS can integrate easily.
In most cases, it is just a matter of changing the endpoint and credentials. There is no need to redesign your architecture or rewrite your applications.
IBEE vs AWS for Healthcare: Where It Shows
The cost difference becomes clear in real usage, especially around data access.
Take a diagnostic chain storing about 500 GB of imaging data. With regular access from radiologists and clinicians, monthly egress can easily reach 300 to 800 GB.
- On IBEE: ₹2 per GB → ₹600 to ₹1,600 per month
- On AWS S3: typically ₹2.35 to ₹2.4 per GB → ₹705 to ₹1880 per month
Even at this scale, the savings are noticeable. As usage grows, this gap increases further.
But the bigger difference is not just cost, it is compliance.
With increasing focus on DPDP Act, ABDM, and data audit requirements, simply saying “our data is in AWS Mumbai” is often not enough. Healthcare organisations are now expected to clearly explain data jurisdiction and control.
IBEE solves this structurally, not through configuration.
Built for the Compliance Obligations Indian Healthcare Cannot Ignore
DPDP Act 2023: Data Fiduciary Accountability
Healthcare providers and healthtech platforms fall under the category of data fiduciaries in the DPDP Act 2023. This means they are responsible for how patient data is stored, processed, and shared. When the infrastructure is owned by a foreign entity, it creates a grey area in accountability that is not easy to justify. With IBEE being an Indian entity, the chain of responsibility stays clear and aligned with the Act.
CERT-In Directions,180-Day Log Retention in India
CERT-In guidelines also require organisations to store system and access logs for at least 180 days within India. IBEE’s logging infrastructure is fully based in India, which makes it easier to meet this requirement without additional complexity.
ABDM Integration: Digital Health Infrastructure Compatibility
The Ayushman Bharat Digital Mission is shaping how digital health systems will work in India. As these standards evolve, platforms will be expected to follow stricter data governance rules. Infrastructure that is already India-based fits more naturally into this direction.
NHA and State Health Authority Compliance
On top of that, compliance requirements from the National Health Authority, state bodies, and insurance integrations are becoming stricter. Many of these indirectly expect data to stay within India. Using IBEE helps simplify this process because the compliance story is already aligned.
Your Patient Data Deserves Infrastructure Built for India
At a broader level, the healthcare organisations that handle this transition well are the ones that make the infrastructure decision early. Waiting until an audit, a compliance question, or rising cloud costs force the change usually makes things harder.
IBEE offers a setup that is built with these needs in mind:
- Patient data stays fully within Indian jurisdiction, with clear audit trails
- Tier 4 reliability supports critical healthcare workloads
- Simple pricing avoids high costs from frequent data access
- Full S3 compatibility works with existing HMIS, EMR, and PACS systems
- India-based support ensures faster and more relevant help
Whether it is a hospital moving from on-premise systems, a healthtech startup building from scratch, or a diagnostic chain managing imaging data across cities, IBEE is designed for how healthcare infrastructure actually needs to work in India.
Get Started — No Commitment, No Complexity
No credit card. No subscription. No minimum commitment.


